It’s been quite a long time since I was a brand-new hire in a flight program and almost five years since my most recent new-hire experience, but I’ve recently been thinking quite a bit about the process of being a new guy in this setting. Part of that reason is that I’ve been flying a lot less in the past year than I have in the preceding years and I’ve been feeling a bit out of practice. I’ve had the sense that I may need to reengage with some of the things I used to do when I was green in the field. And while I’m at it, maybe there’s some value to others if I share the details of that process.
One of the toughest parts about starting out in the flight world is learning protocols. This is true for folks who have never flown before, but also relevant when moving between programs. In particular, it’s the drug doses that have always seemed the most important. While it’s more or less acceptable these days to check doses on the phone as needed, I’ve always been of the mindset that it’s worth memorizing the important and commonly used ones. To help with that, I put together notecards for my drug doses. I have these notecards on an app on my phone called AlgoApp (formerly AnkiApp). I’ve also copied them into a similar app called Brainscape. If you’re interested, check them out here:
Download files for AlgoApp (requires a bit of work to upload into your own account; if that doesn’t work, just get in touch with an email and I can send a link directly)
Download deck directly from Brainscape
And for what it’s worth: I prefer AlgoApp/ AnkiApp for my own use because the formatting looks better and has some nice extra features, but Brainscape is much easier to share between/ amongst folks because it allows you to create links directly to decks.
I built these cards the last time I came back to flight, almost five years ago, but haven’t used them much in the past few years. That said, I’ve now taken the time to update them, check for errors, and now they are there for me to use as needed.
Another potential strategy for learning protocols and the specifics beyond just the drug doses is creating “scripts” as discussed ages back in one of my first podcasts with my good friend Richard:
Scripts Discussion with Richard
While I never did this with all my protocols as Richard describes, I did create a script for rapid sequence intubation (RSI):
I had every intention at that time (which was 2021 or so) to do something similar for other high-risk, low-frequency procedures, but I never did get around to it. As a way to re-engage with this process, however, I’ve created a few more of them while writing this. The difference being that these are more generalized and less specific to one job setting, as I now spend a lot of my time outside of the flight job, in settings where a specific kit or bag is not always guaranteed.
The way I used to engage with the one RSI script that I did build back then was to listen to it occasionally on my drive to work. That said, I think most of the value was in creating the thing and spelling out each and every step explicitly. This is to say that just listening to my recordings likely doesn’t offer much benefit, rather they are just here as examples for what you can do yourself.
And while this is something that I’ll probably never take the time to do, a video version of the thing would probably be even higher yield, as coordinating the physical movements and actions with other humans is a key component to actually doing the thing in real life.
Moving on, one other thing that most new clinicians are great at and that I have grown lax with is knowing where precisely every piece of gear lives on the unit (helicopter, in my case). I’ve always been a bit OCD about daily checks, but with time it’s seemed to have shifted to just checking the main cabin and not the stuff in the back. Or just quickly laying eyes on the macro components, but not opening each specific pouch.
It’s also true that things change over time. How the aircraft is set up now is different than how it was when I started. And there are good reasons for this: best practices change, setups get modified for new equipment, new folks at a base have different preferences, arbitrary changes from above, etc.
So the thought experiment here is how to re-ingrain gear/ kit organization in my mind so that I don’t reach for where things used to be. One thought was to identify very specific patient cases in which I’d have to use certain things and map out where I’d go. Sort of revisit the script concept in a slightly different context.
So for example: Let’s say we have an OB case with imminent delivery. Which bag does the OB kit live in? Or the doppler? And which pocket in that bag for each?
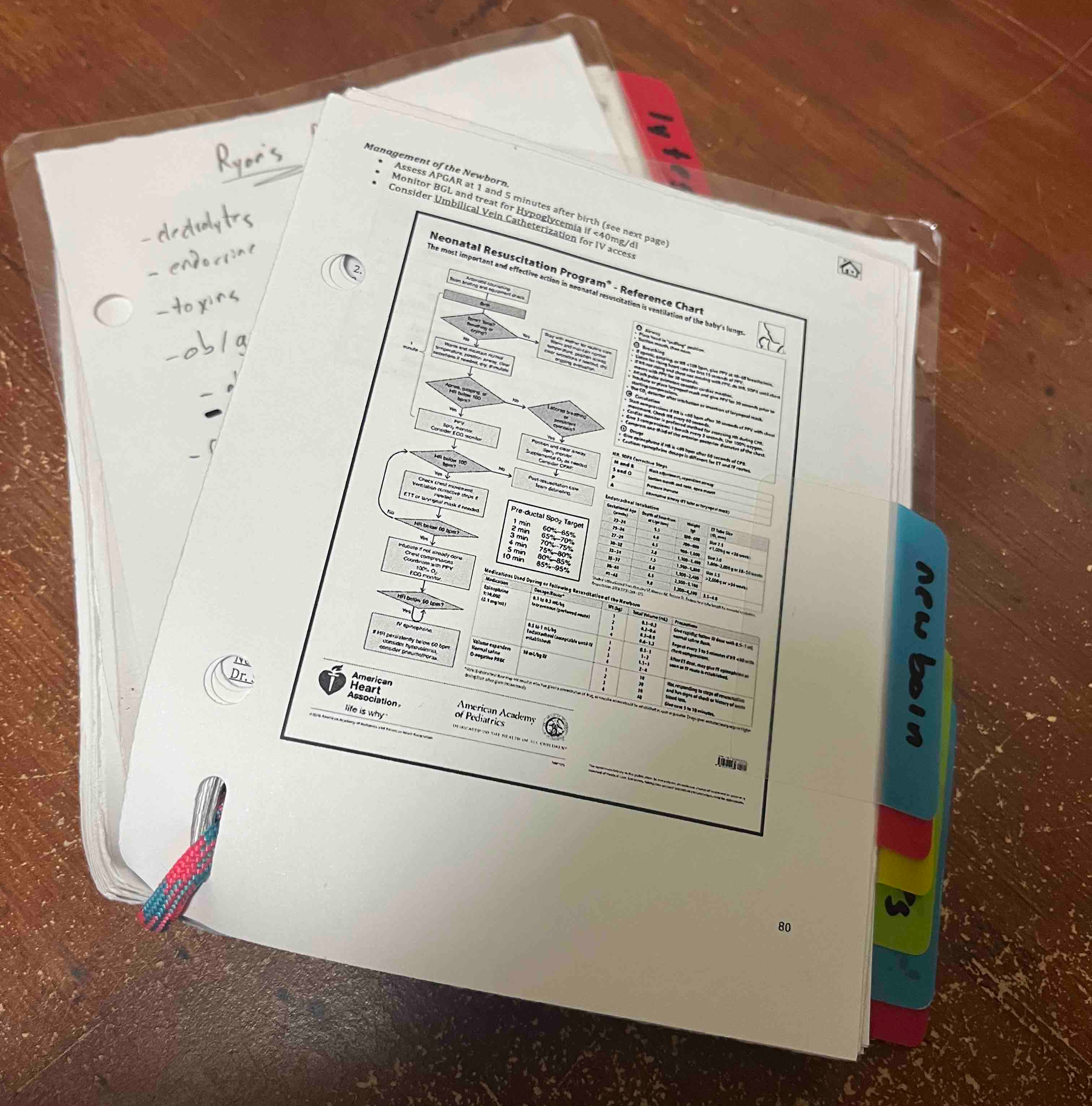
And the baby is delivered, but needs ventilatory support. How deep down in that main bag is the infant BVM? And where are all the miscellaneous pieces to set up the HFNC system if we want to go that route?
Then for creativity’s sake, let’s say we break down and an EMP takes out our EZ-IO and we live in a world where we won’t get fired for catheterizing an umbilical vein - where do I find the closest 6F feeding tube and an IV start kit? Is there one in these bags I already have open or do I go to where I usually grab one of these things? And what can I use to tie off the stump after the line has been placed to prevent bleeding?
Umbilical Vein Catheterization Reference
(More on that idea on the website at the Protocols & Cheat Sheets page)
And now! Let’s say mom is bleeding real bad. Which side flap of the med pouch has the TXA? And in which row? Because I want the helpful first responders on scene to both get the drug quickly for me and recognize that I know my gear.
Etc. This sort of thing. Except I actually answer all the questions instead of just pointing out what I think I should know.
And also I can work through the process in different settings, depending on where I am working at a given time.
Next thing: I linked above to a document I made for a totally different flight program years ago. It’s an abridged version of protocols/ treatment guidelines we had, designed to be a quick reference for use in the field. I still keep a few of the sections from that document printed out and in my flight suit, I just have edited the specifics to reflect my current program’s guidance:
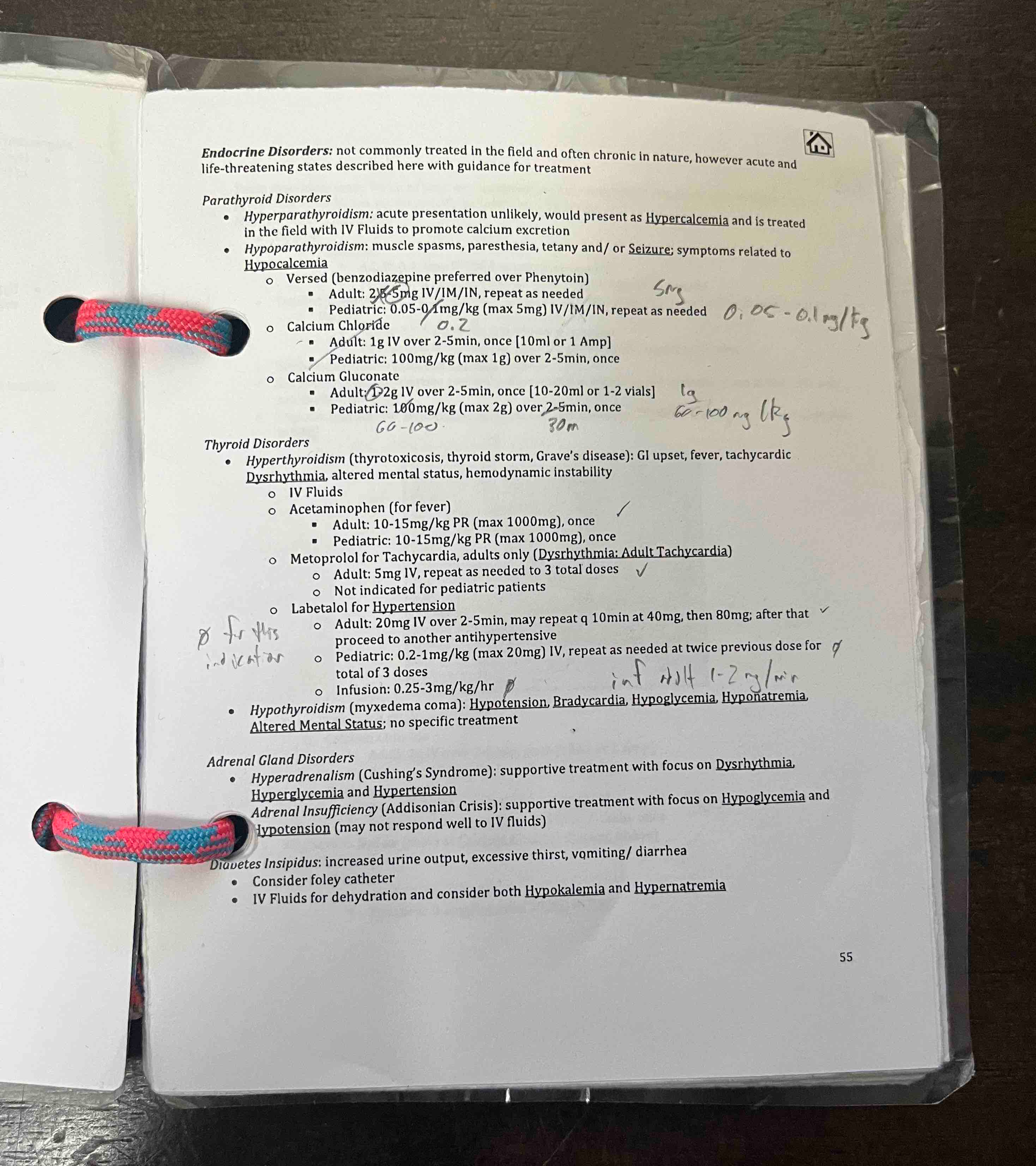
I haven’t updated that for quite a while, but now it’s in the works. I also have been sitting on a few updates to the collection and have finally made time to finish them:
So here’s what it looks like now:
Part of the reason, I think, why all of this (not just the reference guide thing just described, but also the notecards and scripts and pretend scenarios - the whole thing) takes so much effort is that the pressure to perform well, that eustress that most new flight clinicians feel, just doesn’t exist for experienced folks after some time. Nobody quizzes us on things, nobody questions us, nobody holds us accountable, etc. Which is fine and it all makes sense to some degree, but it creates an environment in which it is very easy to become complacent.
So there you have it. A few things I’m doing to get back to being an above-average employee at my part-time flight job :)