The patient was a 4-year-old female being transferred out of a conflict zone for care in another recipient country. Patient had known history of Tetralogy of Fallot (ToF), needing follow-up care with pediatric cardiology unavailable in host country.
She was being transported by another ambulance crew in a convoy of many ambulances, multiple patients were being transferred out of the region. While holding the convoy’s position at a safe crossing point, med crew was summoned to check in on this patient.
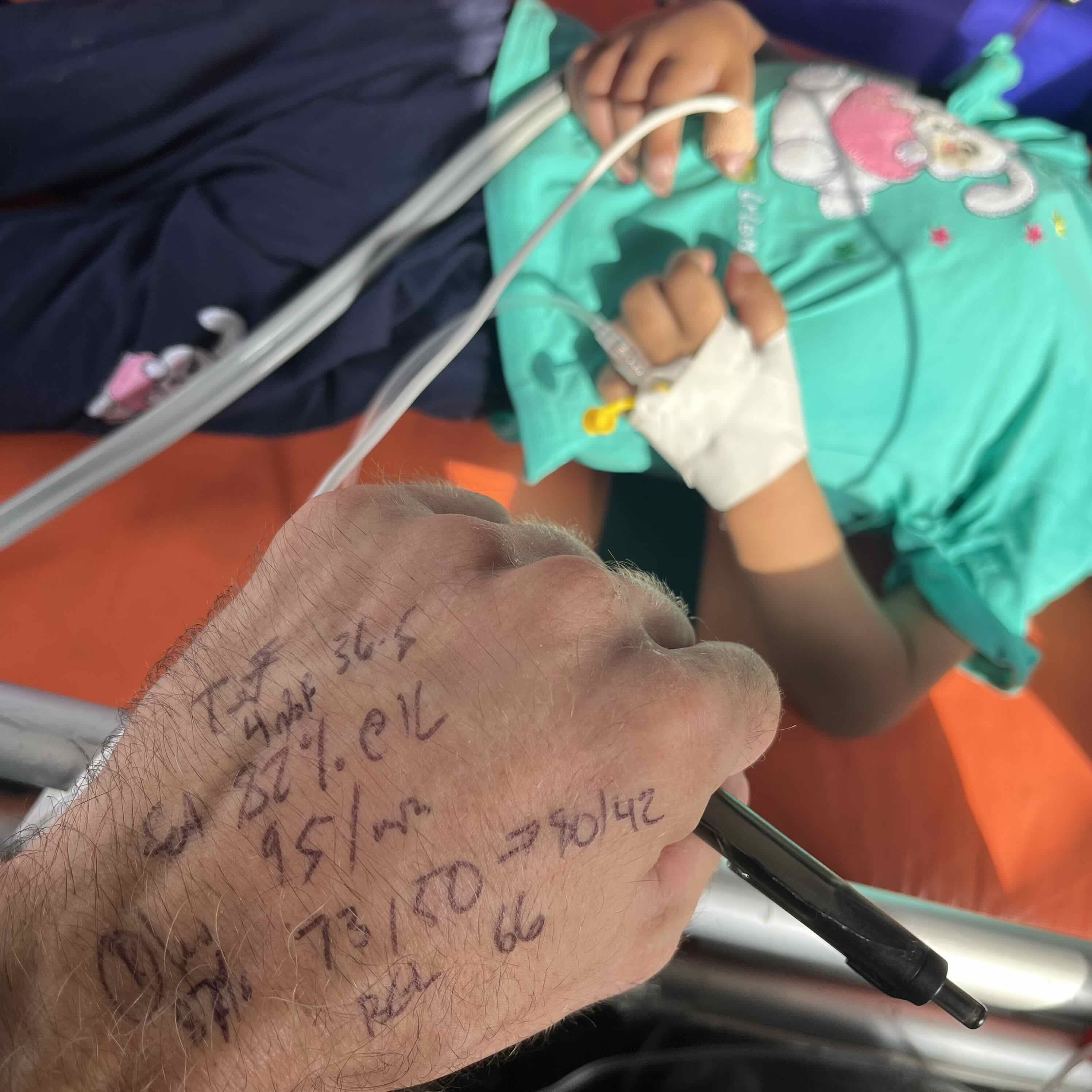
Patient was stable on assessment, no distress and no cyanosis, but hypotensive and with a low SpO2 at both right hand and the foot. The other crew that had transported the patient up to this point had already initiated oxygen at 1lpm.
Now the goal of treatment was to ensure that the patient was and would be stable enough to make it across the border and to a receiving ambulance on the other side. There was some concern that if care needed to be escalated (i.e., with pressors or any form of machine-assisted ventilatory support - anything beyond a nasal cannula) she could lose her ability to be evacuated.
There wasn’t much available in terms of medical history. ToF was a known diagnosis, but there was no information about surgeries or baseline oxygen saturation or known complications.
The decision was made to administer IV fluids in 100ml increments (which was just shy of 10ml/kg) to support her blood pressure and to discontinue oxygen to both establish a baseline and limit unnecessary treatment (to improve the chance of success in getting her across the border).
Now the patient did just fine on ambient air and the blood pressure improved with fluid boluses (three in total). She was, in fact, able to cross and exit out of the region without issue. SpO2 stayed in the 80s, did not cross below 80; it also did not get above 89. Beyond that, there is no way of knowing more about her outcome.
Questions during and after the case included the following:
- Does the concern for oxygen causing closure of the PDA still persist at 4 years?
- And when is it justified to give oxygen to a patient with ToF/ in a case like this?
- Is there a normal SpO2 range for this sort of thing? It is likely highly variable and based on patient’s specific history, but is there a ballpark for when this is not known?
- How much caution is needed with IV fluids in ToF?
Now before diving in to all the details, a quick review of the pathophysiology:
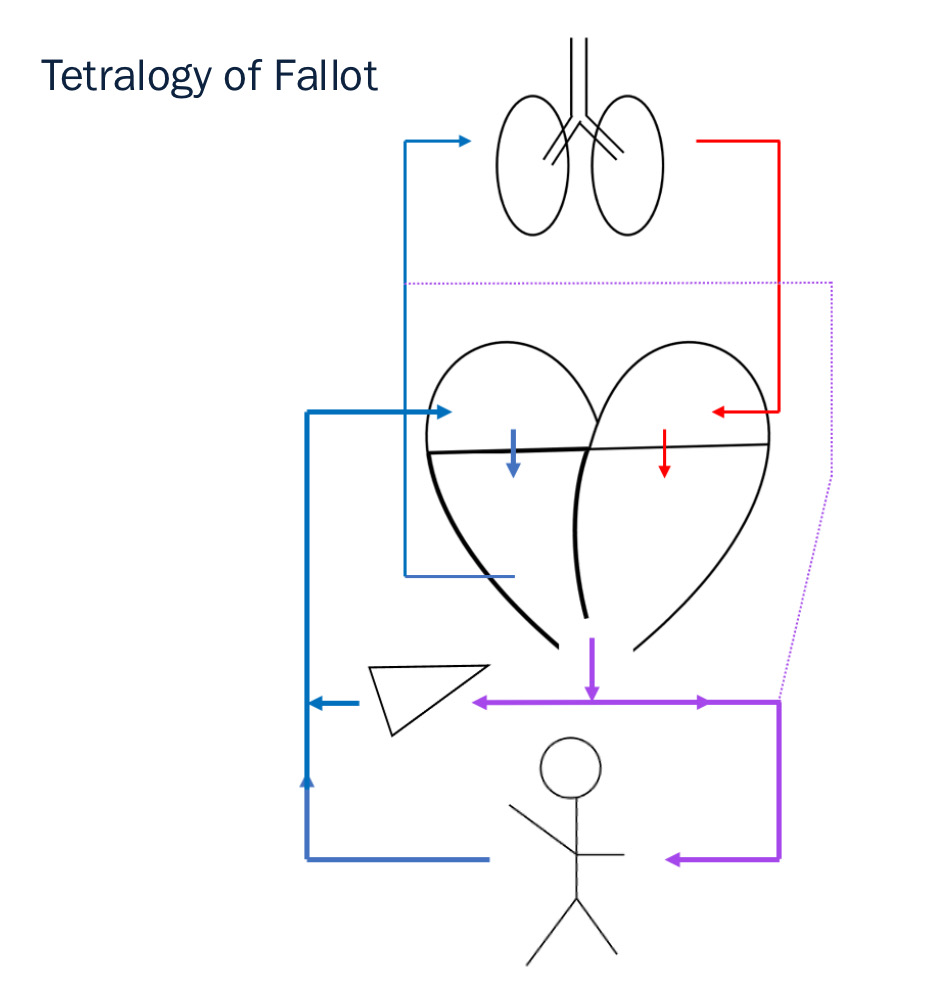
(these sorts of stick figure graphics to describe hemodynamic states are discussed in another blog post: Hemodynamic Sketches)
ToF is composed of the following four things, all present at birth: ventricular septal defect (VSD), pulmonary stenosis, right ventricular hypertrophy, and overriding aorta (which means the aorta’s origin/ blood flow comes from overtop the VSD, not just from the left ventricle as is normal). The result is that blood going out to the body is mixed or not fully oxygenated, hence ToF is considered a cyanotic heart lesion or defect.
Now the pulmonary stenosis part of this means that blood flow out of the right ventricle to the pulmonary artery is limited. There is some collateral flow from the aorta via the PDA to the pulmonary artery (left-to-right shunt). Classic teaching is that oxygen given to “ductal-dependent lesions” can cause premature closure of the PDA and worsen outcomes
Normally the ductus arteriosus closes at birth. It is designated a PDA when needed for survival (i.e., a “ductal-dependent lesion”) or when it persists into adulthood. Now in this case with a pink (well-perfused) 4-year-old and the benefit of hindsight, it is most likely that the PDA associated with her ToF has long-since closed. While it could be the case that she had surgery to keep it patent, that is unlikely in the absence of cyanosis, especially at this age. It could be assumed that her case sits left-of-center on this graphic representing the spectrum of ToF:
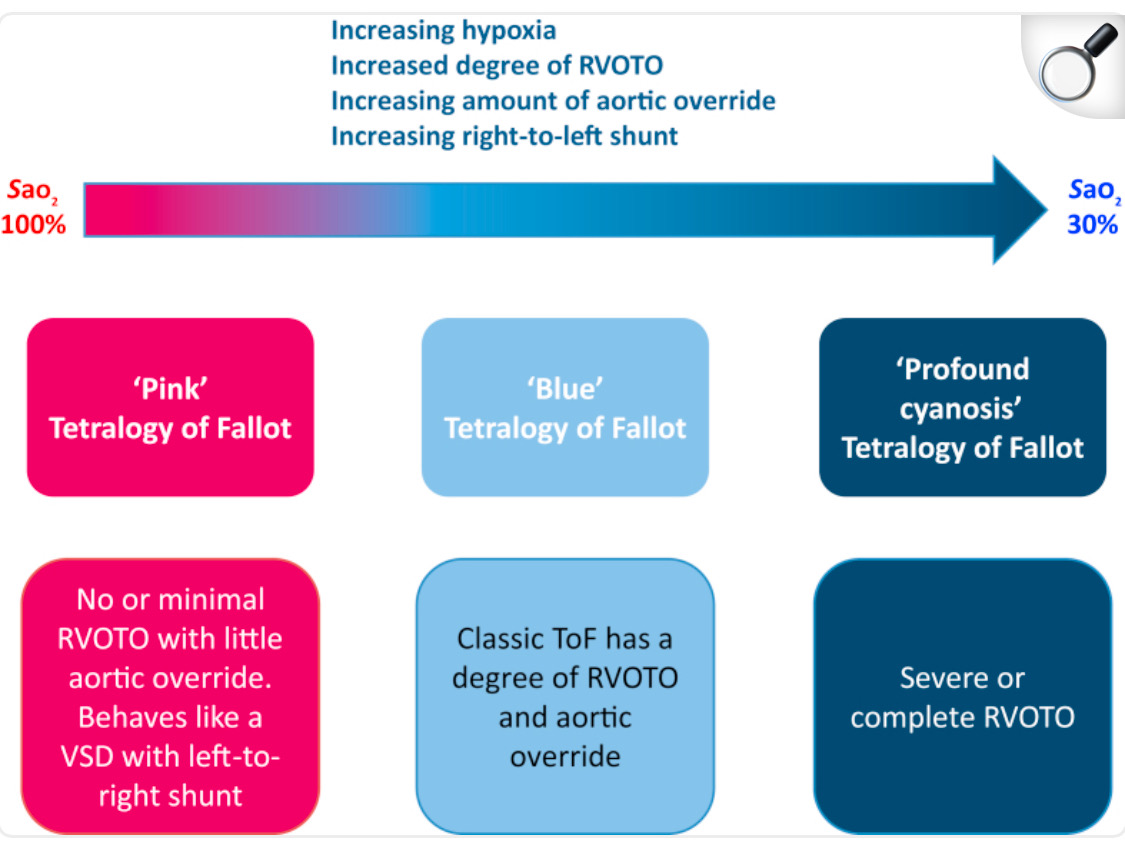
So withholding oxygen to prevent the closure of a PDA in this case wasn’t necessarily the right move – it would have been totally fine to give oxygen if needed. That said, SpO2 change with supplemental oxygen would be dependent on the severity of the disease and there may not have been much of a change with more oxygen. She was on 1lpm at the start and maintained those low sats on ambient air, but could have had a better SpO2 with more oxygen.
As far as normal ranges or a goal to target in the absence of a solid history, it is highly variable. There is some literature suggesting SpO2 as low as the 70s is “normal” for a ToF case, but beyond that it is difficult to identify an SpO2 goal. That said, the alternative is to use different assessment parameters: color, capillary refill, mentation, etc. - all of which were OK in this case.
And then the last question was in reference to fluid boluses in a case like this. Treatment was started at just under 10ml/kg simply to avoid fluid overload. This is always a reasonable strategy when in doubt, but it’s also worthwhile to try and better understand the pathophysiology and potential risks.
The concern with fluid overload and fluid boluses is more an issue with inadequate left heart function. If the left ventricle can’t move fluid out or if systemic vascular resistance is super high and it’s tough for the left side to push things into it, this could result in pulmonary edema. But in this case, ToF is more of a right-side issue and, in fact, fluid is generally well tolerated. Especially in milder or “pink” cases. While it’s always OK to give fluids slower if in doubt, treatment here was probably overly cautious.
And that’s it. One other thing worth reviewing for the treatment of ToF are “tet spells” or acute episodes of severe cyanosis, but that’s a homework assignment and not a today discussion.
References:
^overview & the pink-to-blue graphic
^normal tx for ToF
^old paper, life expectancy w/o sx