Not too long ago we had an interesting case of an elderly male patient who developed a DVT after an injury to the leg with subsequent immobility. The crux of the case was that access to medical care was severely limited by an ongoing conflict and availability of medications. It all worked out in the end, but along the way there were a handful of interesting discussions and a number of learning points. So let’s dive in.
Case Summary:
Day 1: Summoned to see a 70-year-old male who presented with swelling in the right foot. Status post injury with likely fracture one month prior (says that no imaging was done at that time), however swelling was new for the past five days. Stated he had been relatively immobile since the injury, but does walk as needed with a cane. Right leg is tender to touch, slightly cooler than left, swollen but non-pitting, discolored/ bruised. Negative Homan’s sign.

Hx: DM, HTN
Meds: ASA, anti-hypertensive, metformin
Also had been taking both Paracetamol and Ibuprofen PRN.
No respiratory symptoms. Well’s for PE low, Well’s for DVT moderate.
EKG showed SR 90s, pre-existing LBBB, negative Sgarbossa. POCUS not available at this time.
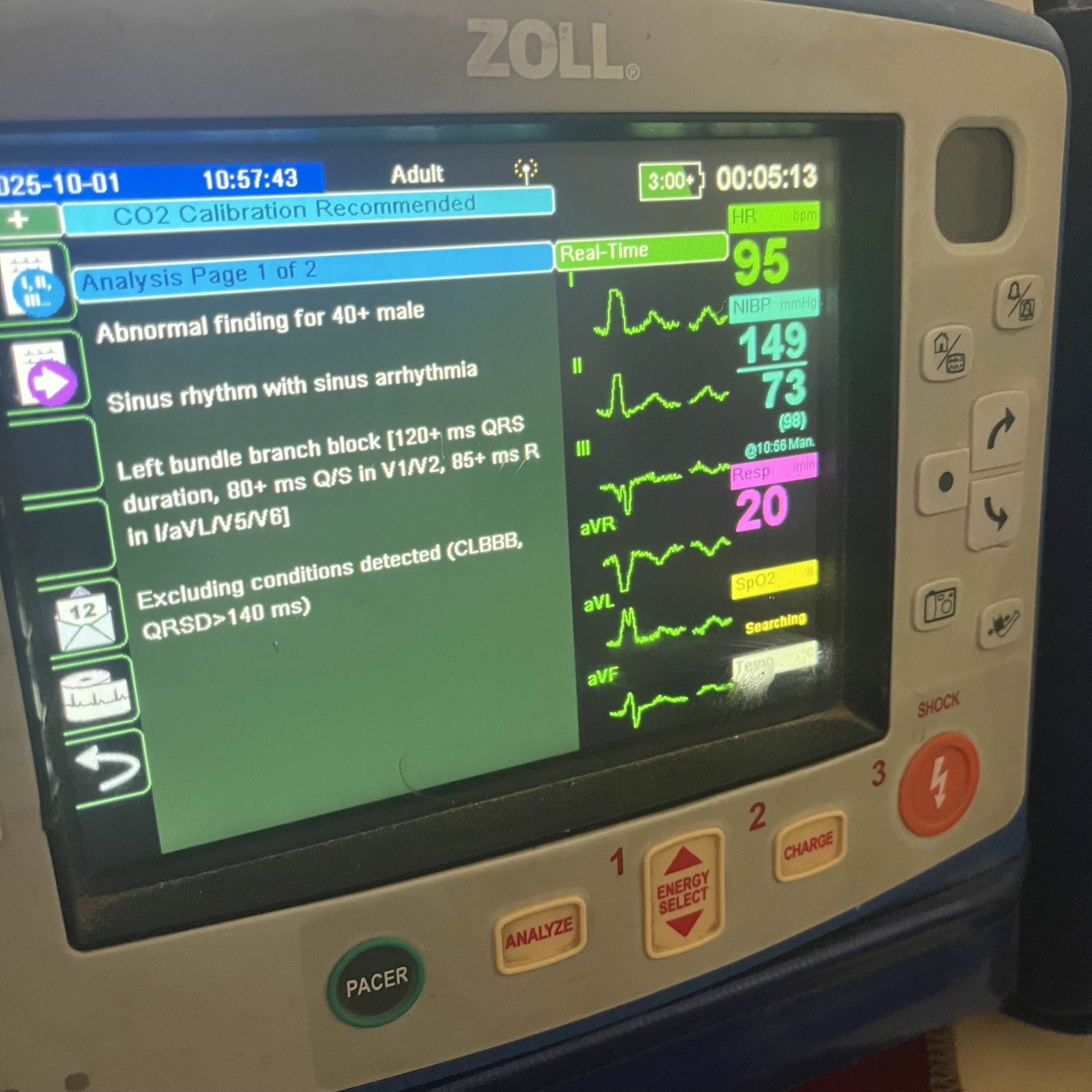
Failed to keep a copy of the full 12-lead… Also see our 12-Lead EKG Reference via the Protocols & Cheat Sheets page on our site for a review of all that.
Day 2: Ultrasound showed non-compressible femoral vein with clot seen inside vessel. Extends from inguinal fold to mid-thigh.
Initial Scan - shows non-compressible femoral vein and clot within vessel lumen
Second Scan - same thing, just slightly better view and a bit slower
Scan of Popliteal area - just to show what the distal bit of the scan looked like
Normally this patient would be referred to the hospital, but that was not possible due to the danger involved with travel. On hand was Heparin 25,000u x1 vial (med bag stock) and Clopidogrel 75mg x30 tabs (patient had acquired “blood thinner” just in case).
Decision made to treat now with 1/2 of the available Heparin SQ (12,500u) and attempt to obtain appropriate agents. Remainder of Heparin to be given that evening as another 12,500u SQ dose while a plan was put in place to source appropriate medications. Clopidogrel not utilized.
Patient’s family was able to acquire Lovenox 80mg/ 8000IE SQ prefill syringes. Treatment initiated that evening.
Day 3: Second dose of Lovenox given that morning. Family instructed in administration in order to continue with the regimen. Plan was to proceed with Lovenox BID until PO meds could be acquired.
Ongoing effort initiated to procure DOAC (either Rivaroxaban or Apixaban) for prolonged treatment.
Resolution: DOAC was eventually acquired and patient transitioned from SQ Lovenox to PO agent after about a week. Repeat US showed clot decreasing in size and no complications reported.
Initial Questions:
Of the available options on Day 2, was treatment with Heparin the best decision?
In the absence of a better way to look into this question, I copied the above case outline into OpenEvidence after the fact and got this reply.
Seems like that was a reasonable course of action, so long as we acknowledge that the heparin dosing wasn’t ideal. We could have considered one full-strength dose vs planned for two sub-therapeutic doses.
Also worth mentioning that giving heparin in the field and without the ability to monitor aPTT levels is suboptimal.
That said, the risk of the big complication (Heparin Induced Thrombocytopenia or “HIT”) with one or two doses is assumed to be quite low, as normally we see it develop after a prolonged course (i.e., >5 days) and more often with IV Heparin (vs. SQ).
And then what could have been done to avoid complications while a treatment plan was developed? Let’s say no appropriate anticoagulants were available?
Turns out there are a few things: compression, limb elevation (when at rest) and early ambulation.
Compression: wrap from the ankle to the knee (i.e., cover the calf muscle) with decreasing tension (i.e., wrap tighter at the foot/ ankle and less tight proximally); ACE bandage is an OK option that most EMS folks would have access to, other elastic bandages may be better; no need to cover the thigh/ clot itself, as the mechanism hinges on calf muscle function to resolve edema and improve blood flow; maintain compression until transition out of the austere setting (may be utilized long-term), will likely require regular re-application with patient movement.
Discussion on knee-length vs. thigh-length compression
Limb elevation: while at rest, keep the affected limb elevated when possible; this facilitates venous drainage and reduces swelling/ pressure.
[Physiologically sound and more or less universally accepted, no direct data on benefit in DVT, especially in the absence of concurrent pharmacologic therapy; that said, very low risk and reasonable to do.]
Ambulation: move the body early; this can be ambulation or passive range of motion exercises (for patients who are immobile); the risk of “breaking up a clot” and causing a pulmonary embolism is not generally a thing (except in the uncommon incidence of a free floating thrombus) and most clinical guidelines now recommend activity over bedrest.
Discussion of bed rest vs. early ambulation
Discussion of exercise after DVT
Free floating thrombus (also note that this free-floating thing can be appreciated on ultrasound)
Further Learning:
Brief Overview of Homan’s Sign
Article on Diagnosing DVT that Covers Well’s Scores
POCUSGeeks Video on Ultrasound for DVT
Comprehensive Overview of Anticoagulation
Follow-Up Considerations:
How reasonable is it to carry Heparin in the prehospital/ out-of hospital setting?
There’s pretty good evidence for benefit of prehospital use in acute myocardial infarction: see HEPARIN STEMI Trial
And there’s been some discussion over the years about prehospital use of heparin for pulmonary embolism: article in EMS World that mentions this
Which seems like a fair extension of data from the ER setting: Early Anticoagulation and Reduced Mortality in PE
Other potential use cases would be acute limb ischemia or atrial fibrillation with an observed embolus (for the POCUS folks). Maybe also a bit of a stretch use case in frostbite for those located in remote and cold areas that also have thrombolytics.
In summary, it seems like prehospital Heparin makes more sense the further we get from definitive care and the more advanced our scope of practice (i.e., ultrasound, thrombolytics, etc.). Probably not all that relevant for most EMS agencies.
How likely is a DVT to develop in an austere setting, such as in prolonged field care or after a backcountry injury that leaves someone immobile while pending evacuation?
As above, I simply fed this question to OpenEvidence and here’s what they had to say.
TL;DR is that dehydration, TXA use and the nature of injuries seen in these settings (multi-system trauma and lower extremity injuries) all contribute to DVT risk.
So definitely a concern and for sure something to think about.
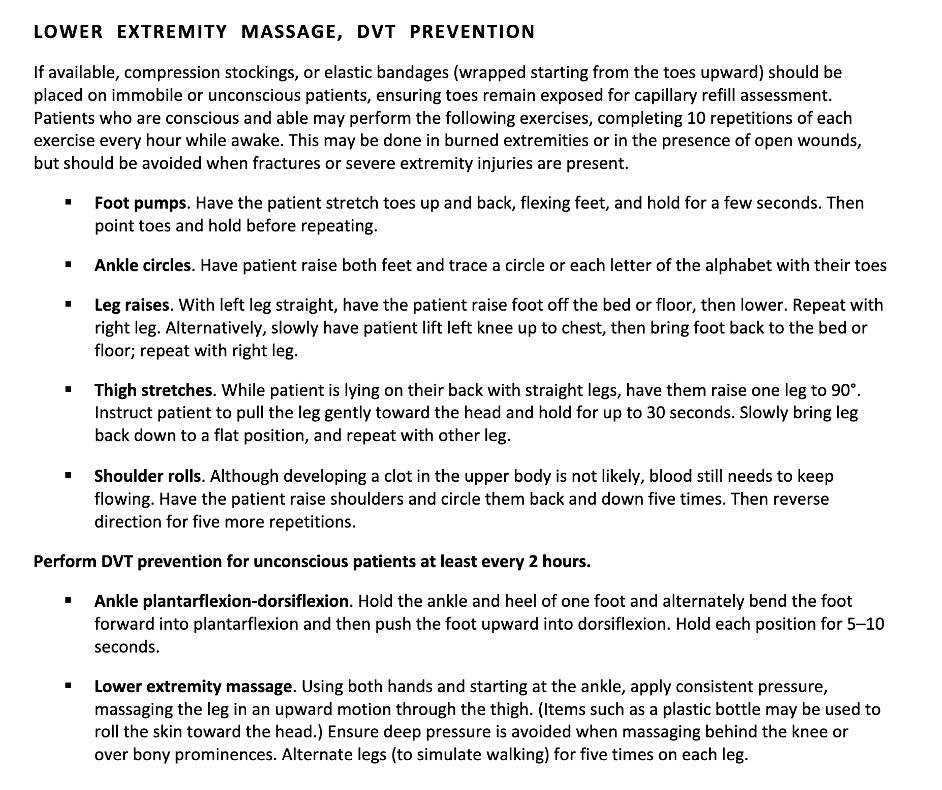
On that note, there is some discussion of DVT prevention in Nursing Intervention in Prolonged Field Care - worth a review of specific techniques outlined there.
Basically take care to mitigate the risk of developing a DVT with physical movement when resources allow, saves the trouble of having to treat the thing later on.
Summary:
DVT is one of those things that we don’t focus on much in the EMS setting where hospital-based definitive care is readily accessible, but in the austere setting it is more likely to come up. Diagnosis can be narrowed in on via clinical history and physical exam, and then confirmed by ultrasound. As for treatment: while anticoagulation is eventually needed, there are a few other things that can be done by medics in the field until that becomes available or concurrently.
As always and forever, let us know if you have any questions or feedback!