Let’s start with a case overview. Extremely detailed dispatch info was: inter-facility flight request for a patient with sepsis, magnesium infusion running.
Differential based on this information alone includes two broad categories: something labor-related (pre-term labor, pre-eclampsia/ eclampsia, etc.) and marked bronchospasm (perhaps also asthma or COPD with concurrent sepsis). Could also be Torsades or hypomagnesemia, but those seem a bit less likely.
Now those two things (something labor-related and marked bronchospasm) are very different, but both involve the use of mag sulfate and sometimes those doses get confusing (depending on your agency), so it’s worth reviewing that sort of thing en route.
Mag sulfate is most commonly described as a smooth muscle relaxant. The way it works is by “increasing the uptake of intracellular calcium into the sarcoplasmic reticulum” (Yartsev, 2025). That said, it also has other effects as well (mainly CNS depression). It is most commonly given as either a timed or continuous infusion. We don’t give it by rapid push because there is some concern that mag can cause either respiratory depression or marked hypotension leading to cardiac arrest - a push dose could theoretically make it happen quite quickly (Patel, 2026). And then we occasionally see it given as a nebulized agent, although this is pretty uncommon.
Typical dosing looks like so:
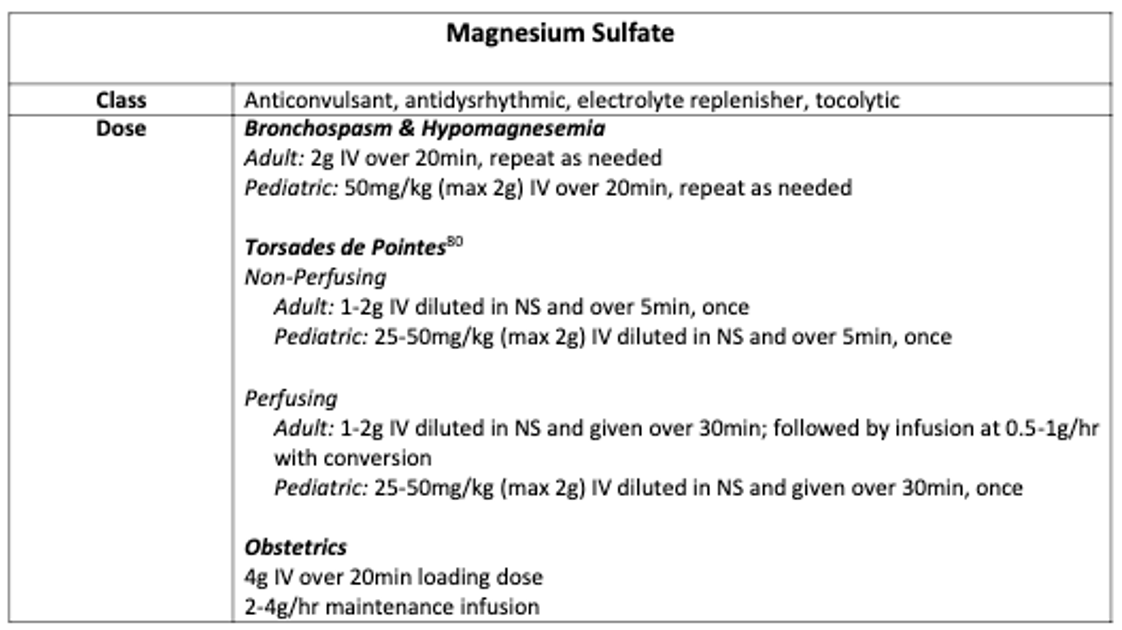
(and that screenshot is from the Medication Guidelines page on our site)
Anyways, report on arrival for this call is that the patient is presenting with post-partum pre-eclampsia. She gave birth one week prior - home delivery into a toilet, patient was unaware that she was pregnant prior to giving birth. History of polysubstance abuse. The baby was resuscitated and held in the NICU (still there at the time of this call) and patient left AMA shortly after delivery. Patient presented on this day with abdominal pain increasing in frequency since delivery. Assessment revealed hypertension (with SBP >200), abdominal ascites, and an H&H under 5&15; crew was also told she had “an edematous labia.” Patient had been given Labetalol twice and had blood products running.
Working through these concepts in sequence, we’ll start with hypertension. Hypertension in and shortly after pregnancy is often described as living on a spectrum with eclampsia (involving seizures) being the extreme end:
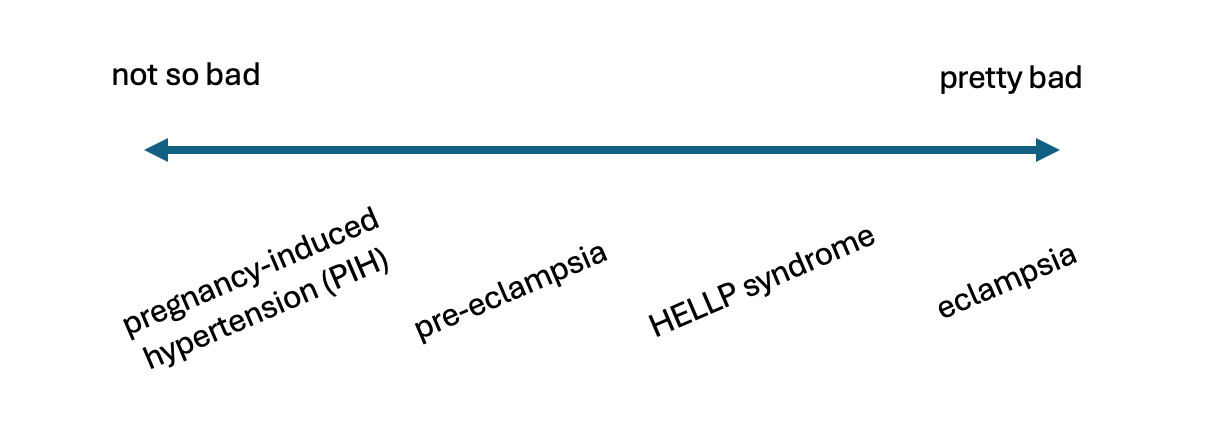
That said, there is some discussion these days that pregnancy-induced hypertension and pre-eclampsia/ eclampsia occur via distinct pathophysiologic processes: Horii & friends, 2025
And we won’t get into HELLP syndrome here, but more on that and these other pregnancy-related conditions here: Farahi & friends, 2024
Either way, these things typically resolve soon after the cessation of pregnancy/ upon delivery, but can persist for months afterwards. Just a few facts about all of this:
- Roughly a third of eclamptic seizures occur after delivery (Salvi & friends, 2026)
- The vast majority of those occur in the first week after delivery (Salvi & friends, 2026)
- The largest gap reported between birth and eclampsia is 10 weeks (Masai & friends, 2019)
- Pregnancy-induced hypertension, on the other hand, can persist for up to three months (Garovic & friends, 2022)
Diagnosis of pre-eclampsia is often cited as pregnancy-induced hypertension plus proteinuria, but can also include new-onset organ dysfunction. So things like acute kidney injury, RUQ pain from hepatic dysfunction, pulmonary edema, etc. could all indicate a pre-eclamptic state (ACOG, 2018). Basically pre-eclampsia is endothelial damage and organ dysfunction in pregnancy, it’s just most common that this affects the kidneys and, therefore, results in protein in the urine. And then this damage is what causes the associated hypertension. (Magee & friends, 2022)
(Also note that that article from the NEJM by Magee & friends (2022) is a super-comprehensive review of a lot of the stuff we’ve mentioned so far; may be worth saving the pdf for future reference.)
Moving on from hypertension and pre-eclampsia, the patient also has ascites - fluid in the abdomen. This checks out with the working diagnosis of pre-eclampsia, as there is often liver-specific organ damage and dysfunction with pre-eclampsia (as alluded to above; Devarbhavi & friends, 2012)
Other potential mega-concerning causes of fluid in the abdomen in this post-partum case could include a few other things. We’ve tried to summarize them along with the most significant bedside findings and lab things to look for on a quick glance thru labs/ when getting a report at bedside:
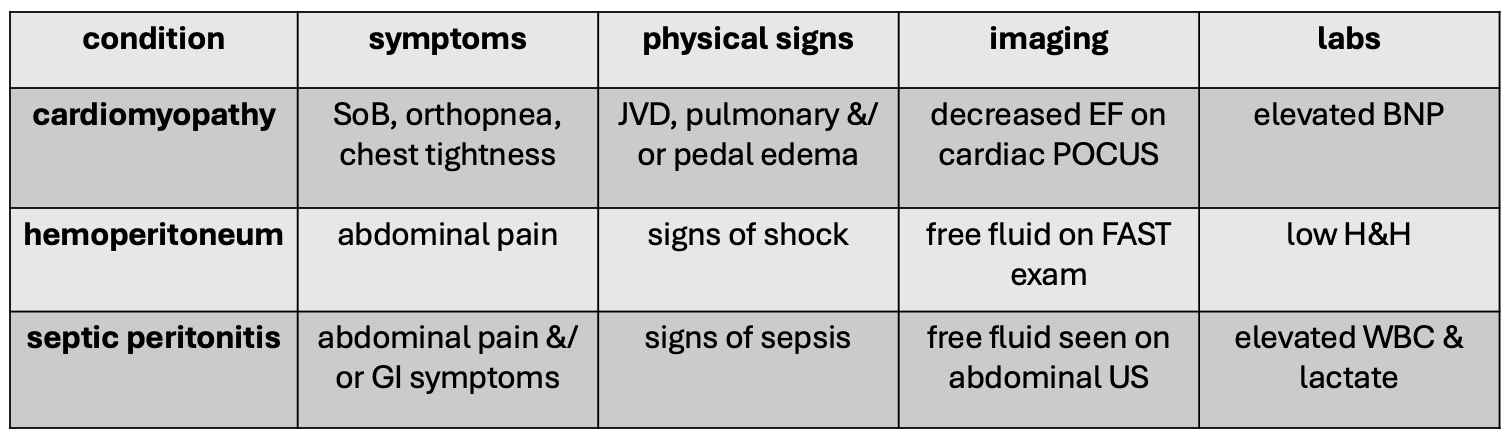
Citations for chart:
- cardiomyopathy - Davis & friends, 2020
- hemoperitoneum - Lier & friends, 2017
- septic peritonitis - Woodd & friends, 2019; Farkas, 2025
(And for a bit of guidance on the citations for “septic peritonitis” above - Woodd & friends (2019) describe the incidence and some of the patho of peripartum infection in general; this could then progress to peritonitis as described by Farkas (2025); just know that it would not be “spontaneous” per se, rather would better be described as “secondary” since a cause/ source is known)
It is worth mentioning, however, that this finding of ascites could have existed before and been unrelated to the pregnancy and delivery. So while it could be a concerning finding associated with an acute complication, it could also be a chronic thing that does not need urgent intervention.
And the last thing to mention from the initial patient report was the low hemoglobin and hematocrit, but no external hemorrhage was reported. We often think of post-partum hemorrhage as having external blood loss, but that’s not always the case. Blood can pool inside the uterus and not escape due to clotting at the cervical os. Or a hematoma can be contained, such as at the vulva or within the vagina. In this case, the patient was reported to have “an edematous labia” which does support the hypothesis of a vulvar hematoma, as blood could have pooled to dependent regions. Confirmation for undifferentiated occult bleed could be done by ultrasound, but may require a CT scan - neither had been done yet. In the case of a vulvar hematoma, however, this is often best appreciated by physical exam.
(And both of these case studies on vulvar hematoma include photos for clarification: Tilahun & friends, 2022; Ayegbusi, 2022)
In any case, the patient was likely bleeding from somewhere and concurrently had marked hypertension and ascites, one week post-partum. Now time for patient contact and assessment.
Patient was responsive to verbal stimuli and oriented to some events. Airway patent, breathing unlabored on supplemental oxygen via a nasal cannula. Radial pulse palpable (yes, do still check pulses on patients!), skin cool and dry, no external bleeding noted. Abdomen was noticeably swollen and tender to light touch in all quadrants (and no, not necessary to percuss the belly…). Labia and vulva were, in fact, markedly swollen - but not to the degree depicted in the case studies cited above. Patient had IVs in both upper arms (as well as a forearm one also) and, therefore, the BP cuff was on the leg. Initial vitals showed SBP around 150, mildly tachycardic HR, SpO2 was fine.
Patient was packaged for transport with blood to continue en route. BP was initially OK at 150 systolic, as treatment begins per local protocols with SBP >160 or DBP >100. That said, repeat BP readings trended up with the highest just after lifting from the sending facility noted to be about 200 systolic. Labetalol was prepared while the reading was recycled. Repeat value was still elevated with a SBP around 200.
Prior to giving the Labetalol, however and fortunately, one of the crew members decided to check a BP at the patient’s arm (as the cuff was on the leg). A second BP cuff was placed on the patient’s upper arm, just overtop one of the IVs that wasn’t being used. SBP of 110. Rechecked, same. It seemed that the patient was not, in fact, hypertensive at all. Just to confirm for sure for sure, that upper arm IV was removed and the reading was repeated with the cuff direct to skin - no hypertension. Just for good measure, the leg reading was done again - still showed a SBP around 200.
What is going on here? Well, turns out maybe a bunch of things simultaneously. First is that the leg BP is often just a bit higher than the arm one (Sheppard & friends, 2019). Also this difference increases (i.e., the leg one gets higher) with worsening peripheral artery disease (PAD; Aboyans & friends, 2012) and PAD is more common with polysubstance abuse (Middlekauff & friends, 2022). And then there is the idea that automatic BP cuffs on most monitors are calibrated to the arm, specifically brachial artery blood flow, and therefore spurious readings can occur when used elsewhere. (Aboyans & friends, 2012).
Now a difference of 90mmHg between the two readings is pretty unusual. Further investigation could have included checking the BP in both arms to rule out any sort of arterial stenosis on the one side - this was not done, however, because the crew wanted to maintain the IV access that they still had. Alternatively, BPs in various locations could have been confirmed manually (although tough to do in a helicopter) or by ultrasound (which may not be available to some crews). And then this could also be a case for placing an arterial line at bedside prior to transport. Regardless, Labetalol was not given and therefore a possible hypotensive event was avoided.
The remainder of the transport was unremarkable and the patient was delivered to the receiving facility with blood products completed and with a reasonable blood pressure measured per the usual method at the upper arm.
Learning points:
- Periodically review mag sulfate doses for various indications
- Pregnancy-induced hypertension (PIH) and pre-eclampsia/ eclampsia can extend quite far into the post-partum period
- Eclampsia is much more than just PIH with proteinuria and may include things like liver injury resulting in ascites
- Not all post-partum hemorrhage ends up external, some is occult or internal
- Maybe don’t trust a blood pressure taken by an auto-cuff on the leg
And very last thing to mention: it was my partner on this run who doubled down on verifying the SBP at the arm; I was prepared to give the antihypertensive based on the false-high leg BP. This was a very good learning point for me and I’m glad I was open to feedback and willing to consider that something was amiss.